What were the issues?
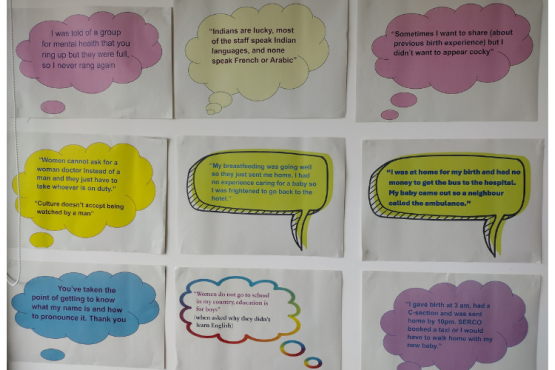
We worked with local voluntary group Carriers of Hope to understand experiences.
Participants had arrived from 11 different countries. Translation enabled non-English speakers to be heard, meaning voices are powerful in the findings.
- It was very hard for the women to navigate services. Women did not get all the care they should have, and pregnancy checks were missed
- Communication barriers impacted at each stage. Services used one size fits all contact approaches that did not meet the needs of vulnerable women who did not speak English and were in an unfamiliar environment
- Costs such as bus fares, dependence on the others for transport and childcare difficulties all lead to lost appointments
- Some women attributed behaviours towards them to racism and lack of cultural awareness
- We also identified issues related to breastfeeding support and barriers to mental health identification.
What has changed?
Improved access, information and services
- New direct email referral route for maternity care for women not registered with GP, overcoming a GP registration barrier for access to services
- New translation support mobile I-pads in the maternity unit
- Better connections and communication between agencies resulting in women getting more help.
- Improved information and communication via work taken forward by Health Access for Asylum seekers and refuges community link workers
- Some of the women interviewed are volunteer buddies for asylum seeking refugee women who are pregnant
Wider impact
The issue of pregnant asylum seeking women being moved to different places in the country during pregnancy has been raised with the Home Office. This fragments their maternity care.
Improved communication and connections between services gives more holistic and effective support. Women and families are less likely to be under the radar of services.
How we did this
Our findings crossed services, so we asked for responses from different organisations via named contacts. We followed up with the hospital, council’s migration team, Local Maternity and Neonatal System and ICB Quality Safety and Experience Committee .
We worked with the City Council migration team and other agencies to plan an inter-agency action focused workshop. Here organisations made pledges and built connections.